|
Contents
Definitions
• DNA
• DNA test
• Gene
• Gene test
• Family tracing
Gene Variants
• Color blindness
• Familial
hypercholesterolemia
• Familial defective
apolipoprotein B-100
• Familial
dysbetalipoproteinemia
• Long-QT syndrome
|
Definitions
• DNA (desoxyribonucleic acid)
DNA is the double-stranded, helical molecular chain found within the nucleus of most cells (exception e.g. red blood cells). The DNA sequence is determined by the sequence of the nucleotides A, C, G, T (A = adenosin, C = cytosin, G = guanidin, and T = thymidin). In the DNA, there are non-coding regions and coding regions. In the coding regions of the DNA, there is the sequence that carries the information to determine the sequence of the amino acids of an entire protein. Hence, by using the information from the DNA, a cell is able to synthesize a protein. |
|
|
| |
|
DNA molecule  |
|
• Professor of Internal Medicine
at the University of Basel, Switzerland
• President of the
Protective Medicine Foundation
• Chairman of
diagene inc.,
an international reference laboratory that
carries out a large variety of gene tests.
|
• DNA test
A DNA test allows to proof or to exclude one or several variations in the DNA sequence from a coding region (gene) as well as from a non-coding region that may or may not cause changes in the function of the cell metabolism. A DNA test can be used to study the inheritance of an individual when compared with other persons that may be or may not be related (e.g. paternity test). |
Correspondence:
Routine Laboratories
diagene inc.
Kaegenstrasse 17
CH-4153 Reinach (BL)
Switzerland
|
• Gene
A gene is the smallest functional unit on the DNA that encodes a protein and enables cell to reproduce and perform its functions. |
• Gene test
A gene test allows to proof or to exclude one or several variations in the DNA sequence from a coding region (gene) that may or may not cause a change in the function of the cell metabolism. As a change in the nucleotide sequence in the coding region has often a direct impact on the sequence of the protein, a gene test allows usually to predict small or large functional changes in the metabolism caused by these variations. |
|
 |
|
• Family tracing
When a inherited disorder is diagnosed in a particular family, further family members can be easily tested by gene tests and the diagnosis of this disease can either be confirmed of excluded. As this strategy to identify an affected individual in such a family is very cost-effective (in autosomal-dominant disorders up to 50 percent of the first degree family members are affected) programs endorsed by the World Health Organization are being carried out in many countries. An example is the MED PED (Make Early Diagnosis - Prevent Early Death) program for familial hypercholesterolemia. |
|
| |
|
|
|
| |
Examples for Functional Sequence Variations Examples for sequence variations whithin genes that cause functional changes. |
|
|
| |
|
|
|
| • Color Blindness |
Color Blindness
Color blindness is a frequent variant defined by the reduced ability to distinguish between certain colors or wavelengths of light. The most common forms of color blindness are inherited and are associated with the inability to discriminate red and green wavelengths (red-green color blindness). This disorder arises from alterations in specific sequence variations in genes located on the X-chromosome, which encode the middle-wave (green) and long-wave (red) sensitive photopigment molecules.
The frequency (or better prevalence) of individuals having color blindness are much higher in males (8.0%), because males possess only one X-chromosome. In females, the prevalence is much lower (0.5%) because the second X-chromosome can contribute the information to generate a middle-wave (green) and long-wave (red) sensitive photopigment protein.
If you have a properly functioning color monitor and you cannot read the numbers within the four circles below, it might be possible that you belong to those individuals that have a certain form of color blindness.
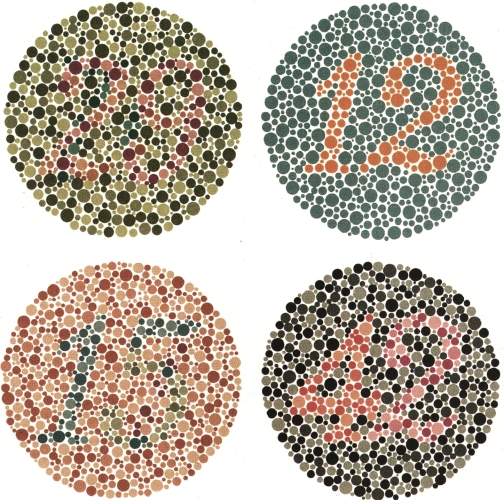
Tables to detect color blindness: you should be able to recognize the following numbers (from left to right) in these four circles: "29", "12", "15", "42". |
|
|
• Familial
hypercholesterolemia |
Familial Hypercholesterolemia
Familial hypercholesterolemia is a genetic disease leadng to two to three times elevated cholesterol concentrations. High cholesterol concentrations within the blood cause typically changes in the blood vessels (atherosclerosis) eventually leading to heart attacks or cerebrovascular strokes. Familial hypercholesterol-emia is due to functional sequence variations in the gene encoding the low density lipoprotein (LDL) receptor. This protein is clearing the blood from chol-esterol-rich low density lipoproteins. When these LDL particles remain in the blood for a longer while, they cause atherosclerotic lesions.
Gene test
An early diagnosis by the help of a gene tests and the early beginning of the treatment in affected individuals can prevent them from heart attacks and strokes. Since the patients have no symptoms from their elevated chlesterol concentrations, identification of family members from families with known familial forms of hypercholesterolemia is crucial. The family pedigree is drawn and the those individuals who might be affected are tested specifically for the mutation causing familial hypercholesterolemia. This concept of
family tracing is an example for the highly successful strategies of protective medicine (see also
PMF, Protective Medicine Foundation). So far, worldwide several hundred functional sequence variations have been detected. Therefore, in a new patient with the clinical features of familial hypercholesterolemia it is necessary to analyse the entire LDL receptor gene. Several laboratories offer a few more common mutations. However, testing for familial hypercholesterolemia means sequence the entire gene to detect so far unknown functional sequence variations. In addition, it is important to compare the results with a comprehensive database containing several hundred known mutations that have been proven to be funtionally important Such gene test are today comercially available, for example at the
diagene laboratories. |
|
CardioVasc 2002;5,11
Familial forms of hypercholesterolemia: familial hypercholesterolemia, familial de-fective apo B, and familial dysbetalipo-proteinemia. (Text in German) |
 |
Kardiovask Med 2004;7,10
Official Swiss recommendations of the Swiss Society of Internal Medicine for the
use of gene tests in hyperlipidemia. (Text in German) |
|
Ger Praxis 2003;8,22,
Review on familial forms of hyperchol-
esterolemia. Special focus on family tra-cing. (Text in German) |
|
Swiss Medical Forum 2002;5,523
The MED PED (Make Early Diagnosis - Prevent Early Death) initiative in Switzerland. (Text in German) |
|
WHO/HGN/FH/CONS 1999 A14
WHO publication on familial hyperchol-esterolemia describing a worldwide initi-ative (MED PED) for the identification of individuals with familial hypercholesterol-emia. (Text in English) |
|
Atherosclerosis Supp 2004;5,1
Review on familial forms of hypercholes-terolemia (Text in German) |
|
| |
|
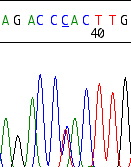
Example of an LDL receptor defect due to an known heterozygous G-to-A mutation, that leads to a stop codon at amino acid position 23: W023X, also called FH Cincinnati-5. Confirmation of the mutation by sequencing of both strands. This mutationexplains the clinically observed phenotype of a hyper-cholesterolemia. The LDL receptor activity is according to the literature between 2 and 5% of normal.
Source:
Original sequence from a patient examined at the diagene inc. laboratories, Reinach, Switzerland |
|
|
|
• Familial defective
apolipoprotein B-100 |
Familial defective Apolipoprotein B-100
Familial defective apolipoprotein B-100 is caused by mutations in the gene encoding the apolipoprotein (apo) B-100 molecule. Apo B-100 is part of the LDL particle and mediates as ligand the up-take of the cholesterol-rich LDL particle into the cell. LDL receptor as well as apo B-100 defects lead to a reduced up-take of LDL particles into the cell and thus, to hypercholesterol-emia. Similar to familial hypercholesterolemia due to LDL receptor defects, cholesterol is elevated within the blood in these patients. High cholesterol concentrations cause atherosclerotic changes and heart attacks or cerebrovascular strokes. The most frequent mutation leading to familial defective apo B-100 is a arginin (R) to glutamin (Q) mutation at amino acid position 3'500 (R3'500Q). A few further sequence variations in the gene encoding the apolipoprotein B-100 were discovered.
Gene test
As the testing for the most common mutations is very simple, early diagnosis by the help of a gene tests and early beginning of the treatment in affected individuals is easily possible and can prevent affected individuals from heart attacks and strokes. Again, identification of family members from families with known familial defective apo B-100 is mandatory (see family tracing, PMF). In a patient with the clinical features of inherited forms of hyper-cholesterolemia, it is very important to analyze the gene encoding apo B-100, the gene encoding the apo E (for familial dysbetalipoproteinemia, see below), and in a next step (because of the more difficult test to analyze the gene encoding the LDL receptor (for familial hypercholesterolemia). |
|
CardioVasc 2002;5,11
Familial forms of hypercholesterolemia: familial hypercholesterolemia, familial de-fective apo B, and familial dysbetalipo-proteinemia. (Text in German) |
|
Kardiovask Med 2004;7,10
Swiss Recommendations for the
use of Gene Tests in Hyperlipidemia (Text in German) |
|
J Lipid Res 1994;35,574
Highest prevalence of FDB worldwide in Switzerland (Text in English) |
|
| |
|
| |
|
| |
|
| |
|
| |
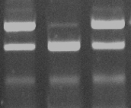
+ - +
Controls Patient
|
Example of a patient positive for the R3'500Q mutation in the apo B-100 gene.
Source:
Original sequence from a patient examined at the diagene inc. laboratories, Reinach, Switzerland |
|
|
|
• Familial
dysbetalipoproteinemia |
Familial Dysbetalipoproteinemia
Familial dysbetalipoproteinemia is caused by mutations in the gene encoding the apolipoprotein (apo) E molecule. Apo E is part of the intermediate density lipoprotein (IDL) particle and mediates as ligand the up-take of the cholesterol-and triglyceride-rich IDL particle into the cell. These defects lead to a reduced up-take of IDL particles into the cell and thus, to a combinesd elevation of cholesterol and triglycerides in the blood. Hence, similar to familial hypercholesterolemia due to LDL receptor defects and familial defective apo B-100, cholesterol but also triglycerides are elevated within the blood. Combined cholesterol and triglyceride concentrations cause atherosclerosis and its complications. The most frequent mutation leading to familial dysbetalipo-proteinemia is an arginin (R) to cystein (C) mutation at amino acid position 158 (R158C) on both alleles of the gene (also called apo E2 allele). Thus, familial dysbetalipoproteinemia is usually inherited in an autosomal-recessive fashion. Several further sequence variations in the gene encoding the apolipoprotein E were discovered and are associated with lipoprotein disorders.
Gene test
Genetic testing for these mutations is very simple. Thus, early diagnosis by the help of a gene tests and early beginning of the treatment in affected individuals is easily possible and can prevent affected individuals from heart attacks and strokes. Identification of family members from families with known familial forms of hyperlipidemia is recommede, although this disease is autosomal-recessively inherited. Therefore the chances to discover an individual affected by family tracing are lower. In a patient with the clinical features of an isolated hypercholesterolemia or a combined elevation of cholesterol and triglycerides, it is important to analyze the gene encoding apo E. |
|
CardioVasc 2002;5,11
Familial forms of hypercholesterolemia: familial hypercholesterolemia, familial de-fective apo B, and familial dysbetalipo-proteinemia. (Text in German) |
|
Kardiovask Med 2004;7,10
Swiss Recommendations for the
use of Gene Tests in Hyperlipidemia (Text in German) |
|
Praxis 2001;90,1297
Familial dysbetalipoproteinemia and the importance of apo E in dementia (Text in German) |
|
| |
|
| |
|
| |
|
| |
|
| |
|
First lane: example of a patient positive (homozygous) for the R158C mutation (=apo E2/E2) in the apo E gene. Second lane: a patient positive having nor a mutation at amino acid position 112 nor at 158 (=apo E3/E3). Third lane: a patient positive (homozygous) for the C112R mutation (=apo E4/E4) in the apo E gene
Source:
Original sequence from a patient examined at the diagene inc. laboratories, Reinach, Switzerland |
|
|
|
| • Long-QT syndrome |
Long-QT syndrome
Long QT syndrome is a hereditary disorder of the electrical rhythm system of the heart. The patients with long-QT syndrome have no symptoms until an often severe arrhythmia occurs that can lead to death. Hence, identification of members from families with known hereditary arrhythmia syndromes such as long-QT and Brugada syndrome is crucial (family tracing). This concept is also another example how gene tests and early treatment can prevent severe complications of a inherited diseqase (protective medicine). Long-QT usually affects children or young adults. |
|
|
|
| |
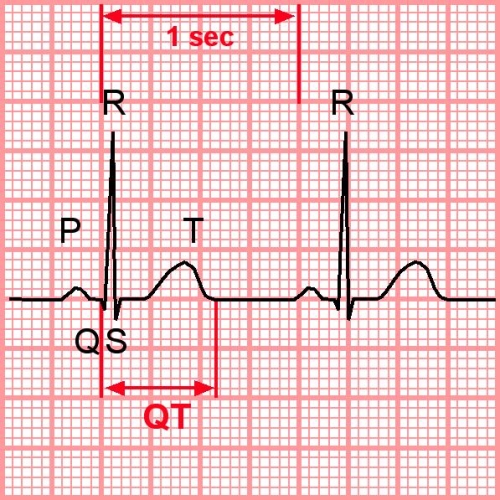
Electrocardiogramm of a patient with long-QT syndrome (a prolonged QT interval 570 msec) |
|
|
|
| |
|
| |
|
| |
|
| |
|
| |
The electrical signal that stimulates the contraction of the heart muscle can be recorded on an electrocardiogram (ECG). A characteristic wave can be deduced; the different parts of this waveform are designated by letters (P, Q, R, S, and T). The interval between Q and T represents the time for electrical acti-vation and inactivation of the ventricles. Patients with long-QT syndrome are susceptible to an abnormally rapid heart rhythm (arrhythmia) which can dramatically disturb the normal function of the heart and lead to death. A specific, very dangerous ECG pattern called "torsade des pointes" can then occur.
The early beginning of the treatment, for example by using beta-blockers, in specific cases surgical procedures or implantable defibrillators, prevents patients from sudden death.
|
|
|
|
| |
|
|
|
| |
Gene test
Since there are often large difficulties to identify the long-QT syndrome solely from measurement of the QT-interval duration on 12-lead ECGs, the role of gene tests in this disease is important. Scientific studies investigating the phenotype of patients with long-QT syndrome show that a normal QT interval (even when corrected for the heart rhythm, QTc) does not exclude this disease. Clinical diagnosis with measurement of QTc may be uncertain in as many as 50% of family members. In a substantial proportion of relatives from Long-QT syndrome families, molecular diagnosis is the most informative method. however, due to the enormous heterogeneity of the molecular basis of this disease, comprehensive screening for long-QT syndrome is difficult and can only be performed in specialized laboratories. Nevertheless, these gene test are today comercially available, for example at the diagene laboratories in Switzerland. |
|
References:
Maron BJ, Moller JH, Seidman CE, et al.. Impact of laboratory molecular diagnosis on contemporary diagnostic criteria for genetically transmitted cardiovascular diseases: hypertrophic cardiomyopathy, long-QT syndrome, and marfan syndrome : A statement for healthcare professionals from the councils on clinical cardiology, cardiovascular disease in the young, and basic science, american heart association.
Circulation. 1998;98:1460-1471. |
| |
|
|
|
|
| |
|
|
|
|
